January 2015: Revision TKA for osteolysis : Dr. Simon Coffey
| 75 yr Female Total Knee Arthroplasty 2004 Excellent Function until 2013 Acute onset Pain |
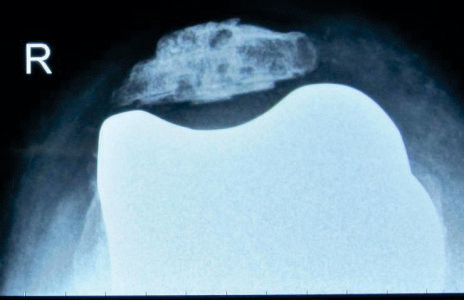
| Xrays |
  Tibial Osteolysis Tibial Osteolysis |
| Radiolucent zone tibial prosthesis bone interface |
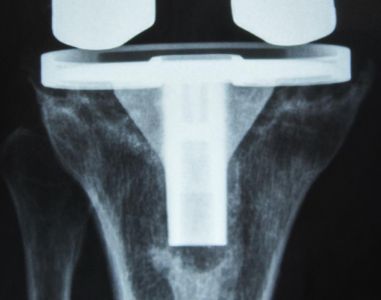 Suggests Tibial Component Loosening Suggests Tibial Component Loosening |
| Diagnosis |
| Polyethylene induced tibial component loosening and osteolysisDifferentialChronic Periprosthetic Infection |
| Management |
 |
| Exclude Infection CRP, ESR, FBC – All normalTc99 Bone Scan Increased periprosthetic uptake in proximal tibia Joint Aspiration Not performed as CRP/ESR normal |
| Surgical Plan |
| Revision TKARemove all implantsDebride and graft OsteolysisSecure new implant fixationLeave Patella if not loose and tracking well |
| Potential Problems |
  |
| Exposure: Osteolysis affects tibial tuberosity – risk of avulsion-take care Cement removal from canal – specialist ronguers Patellar Osteolysis – consider retention over revision. Degree of osteolysis often underestimated on films – prepare for worst case scenario. Stems and or sleeves |
| Operative Findings |
| Extensive polyethylene laden synovitisLoose Tibial Component Extensive mostly contained Osteolytic defects proximal tibia Required augmented fixation with sleeve to re-establish tibial joint line Anterior tibial defect- Tubercle integrity maintained Well fixed femoral component with posterolateral condylar osteolysis Satisfactory fixation with stem and TC3 Femur Patella well fixed and stable – not revised |
| Procedure Outcome |
 |
| Revision Implant-Semi constrained Rotating Platform Uncemented stem femur Uncemented Stem and sleeve tibia, with cemented baseplate Bone Graft to large tubercle defect Patella retained |
| Post Operative Radiographs |
   Good Comfort ROM 0-110 at 6 months Good Comfort ROM 0-110 at 6 months |